clinical pharmacology
FREQUENCY
of arterial hypertension (AH)
AP > 140/90 mm Hg
At elderly 20-30 % in population
Principles of treatment of arterial hypertension
1. Treatment should be started as soon as possible and should be hold till the end of life. Canceling antihypertensive drugs administration causes relapse of AH.
2. All the individuals with increased arterial pressure should obtain drugless treatment (modifying lifestyle):
-rejection from smoking and alcohol;
-increasing of physical activity;
-restriction of salt consumption (less than 6 g per day);
-decreasing of body weight in a case of obesity.
3. Scheme of drug treatment should be the most availably simple – 1 tablet per day if possible; it is better to use drugs with long duration of action (prophylaxis of considerable fluctuation of blood pressure during the day).
4. Rapid decreasing of blood pressure to low figures is dangerous, especially for elderly patients.
5. Main aim of the treatment is to decrease blood pressure to 140/90 mm Hg. To improve life prognosis is the aim that has a more significant meaning than character of drugs used to reach this aim. It is better to prescribe cheap and “non modern” drugs than don’t treat the patient
clinical pharmacology of drugs that controllvascular tone
clini parmacology of cardiac glycosides
clinical pharmacology of diuretics
Treatment of arterial hypertension
Drugs of first row
-diuretics (furosemid, dichlothiazide, spironolacton)
-inhibitors of ACE (captopril, enalapril, ramipril)
-antagonists of angiotesine II receptors (АRА ІІ) (losartan)
-β-adrenoblockers (anaprilin, atenolol, thymolol)
-α-adrenoblockers (prasosine, terasosine)
-α-, β-adrenoblockers (labetolol, carvedilol)
-Ca ions antagonists (niphedipine, amlodipine, verapamil)
Drugs of second row :
-agonists of α2 –adrenoreceptors of central action (clopheline, methyldopa)
-sympatholytics (reserpin, octadin)
-direct vasodilators (molsidomin, hydralasin)
New drugs:
-imidasolines (moxonidine, rilmenidine)
-serotonin receptors blockers (ketanserin)
-monateril (calcium antagonist, α2 -adrenoblocker)
drugs of first row in treatment

diuretics
a/ thiazides
b/ loops
c/ spiranolactone
ca sparing diurtics/k sparing diurtics
d/ osmotic diurtics
e/ low ceiling diurtics
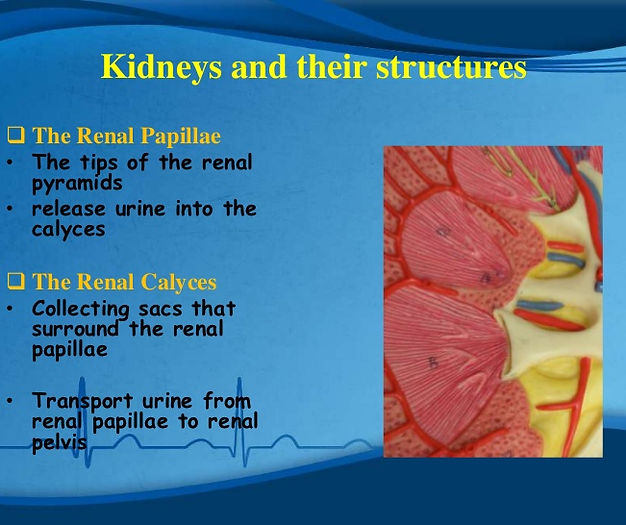
defination and functions
promote urine production
saluretic
induce durisis
action = water+ salt excretion
play a role in reduce blood pressure and so enhance renal blood flow due to hypovolomic
mechanism of action
Diuretics are tools of considerable therapeutic importance. First, they effectively reduce blood pressure. Loop and thiazide diuretics are secreted from the proximal tubule via the organic anion transporter-1 and exert their diuretic action by binding to the Na(+)-K(+)-2Cl(-) co-transporter type 2 in the thick ascending limb and the Na(+)-Cl(-) co-transporter in the distal convoluted tubule, respectively.] Classification of common diuretics and their mechanisms of action.
ExamplesMechanismLocation (numbered in distance along nephron)
–ethanol, waterInhibits vasopressin secretion
Acidifying saltsCaCl2, NH4Cl1.
Arginine vasopressin
receptor antagonists amphotericin B, lithium citrate Inhibits vasopressin's action5. collecting duct
Aquaretics Goldenrod[citation needed],Juniper[citation needed]Increases blood flow in kidneys[citation needed]
Na-H exchanger antagonists
[dopamine ]Promotes Na+ excretionin proximal tubule
Carbonic anhydrase inhibitors {acetazolamide,}]{ dorzolamide } Inhibits H+ secretion, resultant promotion of Na+ and K+ excretion: proximal tubule
Loop diureticsbumetanide,] ethacrynic acid,]furosemide, torsemide Inhibits the Na-K-2Cl symporter. medullary thick ascending limb
Osmotic diureticsglucose (especially in uncontrolled diabetes), mannitolPromotes osmotic diuresis proximal tubule,descending limb
Potassium-sparing diuretic amiloride, spironolactone, eplerenone,triamterene, potassium canrenoate.Inhibition of Na+/K+ exchanger: Spironolactone inhibits aldosterone action, Amiloride inhibits epithelial sodium channels[10]5. cortical collecting ducts
Thiazidesbendroflumethiazide,hydrochlorothiazideInhibits reabsorption by Na+/Cl− symporter4. distal convoluted tubules
Xanthinescaffeine, theophylline, theobromineInhibits reabsorption of Na+, increase glomerular filtration rate1. tubules